 Live Music Archive
Live Music Archive Librivox Free Audio
Librivox Free Audio Metropolitan Museum
Metropolitan Museum Cleveland Museum of Art
Cleveland Museum of Art Internet Arcade
Internet Arcade Console Living Room
Console Living Room Books to Borrow
Books to Borrow Open Library
Open Library TV News
TV News Understanding 9/11
Understanding 9/11tv C-SPAN2 Weekend CSPAN August 3, 2013 7:00am-8:01am EDT
7:00 am
to the bedside and helping patients navigate our incredibly complex challenging health care system. her story is she and her family were overwhelmed by that ventilator, they were terrified of it. if you imagine what it is like hooked up to a ventilator and then anxiety was driving her back to the hospital over and over. the insurance company let her go to a long-term care unit for a little while, enough time for the family to get trained on how to manage the ventilator and form a care team with her primary care provider and palm enologist and she hasn't been back to the hospital. there are certain people who like to be in the hospital. if you are homeless living in tent city, having a flat screen tv and three meals is probably a good thing but for many patients they don't want to be in the hospital and the current system ignores them. 25% of elderly medicare patients are readmitted to the hospital within 30 days.
7:01 am

that is an absolute f to our seniors. people are being thrown off a cliff when discharged from an american hospital because of their medications are changed, they have many tests and follow-ups, they are overwhelmed by what has happened to them. another case, less you think this is just a story of poverty this is a middle class woman and she was in hospital that is part of a five hospital system that is connected electronically so doctors have instant access to the records any time a patit comes back and since 1996 this patient had 102 emergency room visits, 54 admissions to the hospital, 147 cat scans and 73 cat scans of the head. this is one of the cats can. that is enough radiation to increase your lifetime cancer risk and this is the middle class woman with a master's degree. so this is of failure of the american health care system and that is what i have learned and
7:02 am
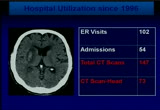
beginning to explore the train of outlaw years of superit utilizes is. as people go more often we ignore them. we don't have a system built to meet their needs. it is a very expensive system as well. i want to tell you how i got started in this. this was my primary care office, my dream to open an office in camden ended is currently boarded up and closed as are many medicaid offices in camden and many primary care offices all over the country and in my time in kansas my rates kept getting cut and at the same time we build new wings on the hospital, expanded the size of the emergency room and i got hold of building data from local hospitals and people like me never get ahold of data like this. this is a summer project by a medical student and let me show you what i found in the data. tivo three competing hospitals so this would be like target and
7:03 am

wal-mart giving you their business intelligence and letting you combine it together. it is rare to put and call care data set together. what we learn from this data set be put in exo which didn't work and still use microsoft excel to analyze this data. we learned half the population of camden uses an emergency room or hospital in one year, someone went 324 times in five years, someone went 113 times in one year. we the public spend $108 million a year for camden presidents, 79,000 people, to go over and over i [talking over each other] over to the hospital. twice as much, we and america spend twice as much as the health care system and we can do amazing things for people but i don't believe we are getting our money's where, $2.8 trillion, 18% of our economy.
7:04 am
i can't get my head around the number that big. i know what that will buy and for 1% of that, you can buy five of me. there are only 15 primary care in camden and all getting boarded up. we have to reinvest the money on the front line of care rather than building more hospitals and expanding emergency rooms, and at incredibly high price if you cut in that and hospitalize and we set a lower price if you talk to people and the market has responded, if you look at every major city those cranes that are above buildings building new lanes and expanding hospitals, if you overpay you will get too much and if we get a bubble of hospital beds and technical capacity of specialists, and we will destroy the other part of the market. and decent primary-care. the most in expensive patients
7:05 am
in camden have $3.5 million in receipts, go to 18% of patients and 90% of costs. we ignore 1% of patients unless you pet scans that are hospitalized and we don't help the navigate the health care system and that is not just the port, this is your grandmother, family member, disabled people with disabilities. the number one reason to go to camden emergency room, head cold. we had 7,000 for ear infection, 7 for violin faction, and i can tell you the public about paying $153, $500. and the racine in my office but paying 10 or 20 times more, if you paid too much for something, that is happening in the health
7:06 am
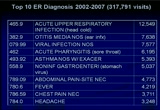
care system. the bulk of patients, and it is a myth of the uninsured, and it is an empty promise, call for an appointment, no one calls you back, that is before the expansion. it will get worse as time goes forward. this is mapping out the claims data. five years of data mapping out the home address of every camden president this is only nine square miles, 6% of city blocks, 18% of patients, 37% of costs. this is just the emergency room and hospital care. all over america, high cost patients are collected in the building. and through state funds and federal funds these other two most expensive buildings in the city, north gate 2, the the beautiful buildings with great
7:07 am
management, 600 patients who are mostly due will eligible, disabled seniors had $12 million in payment for their care to go back over and over to the hospital. the building at the bottom, 300 patients, it is a nursing home, 300 patients had $13 million in payments to go to the hospital. we mapped out they all over the country and found the same patterns in newark, collecting high cost patients. in the state of maine with the help of governor page and commissioner mary mayhew we mapped out three counties and the rural state and as you get older and more disabled is harder to live in the middle of nowhere. they didn't let us show it to you but these are town hot spots that actually get down to the building level. even in a rural state collecting high cost patients and the question for all of us is service delivery innovation. do we want to move those people
7:08 am

around or bring care to them? on want to close with the really important announcement that the fountain of youth has been discovered in pennsylvania. it is not in florida. this is an important study. this is the random controlled child with 1700 patients over a ten year period. we will never have a bigger study to look at population, health and care coordination. this is part of the medicare chronic care demo and in this model is the nurse going out every week or every other week in a very specific data driven-ee model going out and visiting patients and we have a lower risk of death, and over the ten year period the mortality benefit did not taper off. let me repeat. 25% lower risk of death.
7:09 am
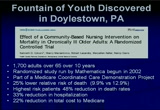
you have to go way back in medical history to find anything with that kind of impact. when we give you drugs, treat your cholesterol, blood pressure is only a few percentage points of impact. this is the early days of polio to beer the days of hiv to see an impact of this magnitude. if this were a pill you would be clamoring for it. the stock would have tripled. the most interesting part of the study is the highest risk patients, the sickest elderly patients had a 50% reduction in the death rate just from having a nurse visiting them every week or every other week. what this story really tells you is we have excess mortality in our broken, fragmented and and coordinated system, 50%. but the nurse visiting your grandmother is enough to drop the death rate by 50%, something is profoundly wrong in today's american health care system. people are overwhelmed and confused and also the highest
7:10 am

risk cohort of 33% reduction in hospitalization and 22% reduction in total cost of medicare. medicare as the demonstration project has tried to pull the plug on the project three time is. most recently so close to pulling the plug they actually had to dismiss the patients unless there was an article calling attention to this in the washington post. sadly, better care at lower costs doesn't have a constituency. medical devices, hospital beds have constituencies. a blockbuster moment in the health care system, we have too many hospital beds in america, a bubble in hospital technology and we have to help this industry make a shift. there had to be a moment in blockbuster video when a young executive said to the executive leadership people are starting to rent videos online.
7:11 am

saying no, we have internal data showing the american public every friday night spends an hour and 15 minutes in our stores. remember that? today they are boarded up all over the country with penny-stock. the story of america is capitalism creates and destroyers and industries become obsolete, hospital beds are becoming obsolete. we don't need all the hospital beds we have. many of you a using bonding authority to underwrite those bonds and doing ribbon cutting for these facilities and every single crane that goes up, every ribbon cutting you do is an invisible tax on your employee benefit program, an invisible tax on every business in your state. we have too much of this. i would like to make a couple suggestions. i believe this is all shifting to the state level.
7:12 am
you regulate these facilities, regulate the providers. everyone who needs to be here to fix the american health care system is right here in this room, governors can take the leadership, states can take the leadership's, all of the most innovative things going on in health care are happening at the state level. you can use your bully pulpit to refrain of the issues and start talking about this in different ways. keep it simple. what i see over and over is we often have cards in our state run systems. you will be moving to managed care and every different constituency group comes and says we don't want to go on managed care. an end lounge carving out wheelchairs' and all sorts of things and your staff can't run these programs. you can simultaneously run contracts, fee-for-service, managed care system. i would encourage you to be all in or all out. pick a system and run it well.
7:13 am

arizona is a wonderful example of this and what arizona did is they are all in. everything is carved in and they actively manage their contracts. this is the procurement problem. if you want to privatize and move to managed care you got to manage those contacts. you can't be a passive purchaser. nurses in cubicles aren't going to have any impact on homeless people with no phones. we are spending a lot of money all over the country on telephone case management models, there is no evidence for them. we got to free the data and use it differently. we have data locked up in so many silos in state government over the health care system. look what happened when the grumpy family doctor got ahold of data. imagine what would happen if we free that they are across the country. there is nothing about this. if lawyers tell you hippo won't let you free the dative they are wrong, they are wrong, they are
7:14 am
wrong. get different lawyers. [applause] >> we have got to build a pathway to support and test innovation. where do i knocked on the door in state government if i have a good idea and proven it? hard to figure out how to navigate state government when you have a good idea. we need a clear path way of how to tester restage ideas, how to test mid stage ideas and bring them through government. it is hard to innovate and to bring ideas forward. the recommendation to push accountability down to the community level. this is a basic concept of accountability. the reason brendon did an amazing job turnaround in new york city police department and new york has the lowest crime rates in the country is he pushed accountability down. he made the precincts, the unit of accountability, the denominator and the precinct captains the accountable
7:15 am
manager. we don't have accountable managers in health care. when there are failures we don't know who to hold accountable. you can't hold your health care plan accountable because they're too far from the point of care. we have to rethink how we push accountability down to the community level, health care is a local problem. we have to figure out, if you're going to procure through managed care we have to actively manage those contracts so they are pushing the accountability down to the committee level. of doctors won't play nice with the hospital, play nice with the nursing home, won't play nice with local dna you won't fix this problem. so thank you for the chance to come and talk with you, i welcome the chance to take questions. [applause] >> first of all, dr. brenner, this was about the most exciting
7:16 am

presentation i have ever heard. i just went through a very tough legislative session where the house bill association, through everything they had at our effort to try to come up with healthier i'll up plans. your remarks resonated with me. how do we overcome the money and clout and connections they have, you have some of the best leaders in the community serving on hospital boards, tremendous amount of resources, nonprofits making a lot of money and build all kinds of buildings. what you said makes whole lot of sense and you as one family practice position put together a really strong case and i would be interested in getting more information because we did get our health and wellness plan
7:17 am

approved. bottom line for the hospitals, just expand medicaid, give us the money and what you have given us is indictment of the present system hasn't worked. it has gotten worse and worse results. my goal is we want to become the healthiest state, how do we get there and your approach makes the most sense and if there is more you can add to it or obviously i would like you to come to iowa. if you can do this in camden, new jersey, i have visited the soup company, i can tell you, camden is that tough place. i have great respect for what you have done and i would be interested if you have got more insight to what governors ken duke to overcome the tremendous clout and power of the hospital lobby. in my previous job we did the
7:18 am

same thing, we had chronic care consortium and finally get to the point that we think we have a plan, the hospital would bail on us because of their bottom line. >> there and a tough spot. i feel an enormous sympathy for the chief financial officers and ceos of hospitals. we need to shift the dialogue. the most dangerous thing in america is an empty hospital bed. and empty cat scanner, it is a cardiologist with an empty slots. that is a capacity bubble problem. we have created enormous capacity that is a bubble. 18% of the economy is home care, a 11% is housing and 7% is fine and. what we have done is create an enormous health care bubble that has to talk at some time.
7:19 am

there is a historic analogue to this, at some point a quarter of state budgets were psychiatric hospitals and your predecessors decided to pull the plug on this and we popped the psychiatric hospital bubble and spent 30 years cleaning up the mess after words. we have to be institutionalized health care and have transitional money to do this. i would say to your hospital's ready, set, go, merge and consolidate because they won't make it as a tiny little hospitals. the next thing i would do is move toward global budgets as fast as possible because their economic model is the same as the hotel industry and the airline industry which is people in bed, volume based game. every day they look and occupancy rates. it is not their fault. the third thing is shift language about this. healthcare's the very messy market. doesn't follow any of the laws
7:20 am

of a normal market. it is akin to a utility. how many train line do you want between two city's? how many water lines for your house? how many cable-tv companies the want to compete to give you cable service? what do you want in iowa city? how many gamma knives the went? how many open heart surgery suite speewun? by allowing them to compete what they are doing is dividing a limited market share, brain tumors where people need open-heart surgery into smaller and smaller groups and the best way for quality health care is to lower the numbers of the procedure you are doing. ironically competition divides the marketplace up, fragmented to the point that delivery is lower quality. this is more can do you to become a you once amazing surgery's, not five doing them.
7:21 am

this is a monopoly problem. we don't have the right language. we failed in this in the railroad, had to have railroads compete against each other and they all went belly up and we do that to the health care industry as well. >> safety net hospitals in the inner city, much different problems in suburban hospitals all of our major teaching hospitals, have billion dollar construction programs, just about finish them. and you have safety net hospitals in the same city of at risk neighborhoods which have severe problems. how do you go to that model for these local safety net hospitals that are in dire straits? >> let's be clear what the data
7:22 am

is telling us, if we scale the project up you would need a third less hospital beds. this is like base closings. we have to abide down capacity and forced mergers and begin to close institutions. the sooner we do that the better off they are, they go under haphazardly. they can't make payrolls, they call you up, people are dying, it is a mess, they have haphazard closures. best thing you do is push a merger and consolidation but if you do that and keep the existing system price will go up. you have to move them towards a different model that is moving toward global budgets. think about a lot of discussion of home savings accounts and using market-based competition, let's be really clear that the
7:23 am

point at which you are on the way to your hospital with your wife who is in labor at 29 weeks and about to have a premature baby. you are not a consumer, you are on the way with your recently born premature baby. you are not a consumer. you are on the way to the gamma knife. you are not opening of consumer reports to see the best value institution. health savings accounts are really interesting and compelling idea but you are talking about essentially healthy people. the point at which you are the most expensive, you are 85 in the last two years of life, you are not in a condition to the consumer at that point. you cannot make a rational decision. >> quick question. one of our biggest issues in all states and so many counties, especially rural counties, the largest employers government and hospitals. you heard the hospitals cut
7:24 am

employment and presented the jobs argument to us at a time when unemployment is high. we are seeing a lot of consolidation of hospitals. the issue is they are cherry picking the consolidation based upon where the least amount of medicaid or medicare patients exist because they are looking for the page people of insurance, people who can pay the bill. how do you d tournament where you have the consolidation? hospitals are using business model to consolidate, not necessarily a community model or health care model. i understand the business equation. that is what it is, a business at this point in time. how do you deal with that this connect? tell us to consolidate but some will be left out because of the cherry picking? >> maryland solved this problem. we had a solution in 35 states
7:25 am

all over the country. weiner added economic downturn in the 70s we did health care rates, regardless of whether you were a medicaid patient, medicare patients or commercial ensure patient you had the same payments at a hospital when you went to the hospital. right now what we have found is you set the payment of love for medicated middle for medicare and high for commercial land they are rushing to grab this pool of commercial patients. do you want fast kind of -- i love marketplaces, i love competition. the want people fighting over commercially insured patients with brain tumors? is that the competition we want? maryland we deregulated hospital rate settings and the only state but still has it is maryland. regardless of which payer you go to the door of the hospital and boston was paid the same amount so we don't want this stuff when we are dividing marketplaces by
7:26 am

payers. the others things that would solve this would-be global budgets for a region and oregon has done that and colorado is beginning to do that and say this is your budget, you need to get your act together and figure out how to spend within this budget. it would be a regional competition. you could mathematically save for this region of the state of delaware you get, currently spend this much and only go 1% a year and if you go above that you won't get it and you have to fight it out among yourselves to figure out how to fix this. is hard to compel people to play nice. at most you can set up a set of rules and you locally can figure this out, then you are going to go belly up. >> given what you said about the way the current incentives work, it is not a hospital's fault, just a game, those are the
7:27 am
rules, and forcing the consolidation? how do you get them to redesign? if you do this oil spill which is great you have a third less hospital bed and is great for everybody except the hospital. what is that strategy? >> it will create different jobs. instead of being the floor nurse you will be, nurse that is the visiting home nurse going to bes homes. what this does is shift to a whole new category of jobs. instead of being in the hospital they will be out of the hospital. instead of the hospital system being a giant hospital and having a very small outpatient footprint you will have a much bigger outpatient footprint and a smaller hospital. these are just economic shifts. this is like at some point steel industry needed to shift its model and you all as governors can play a strong leadership role in your rhetoric and
7:28 am

actions to send a signal to all of them to begin shifting. interestingly when you go to their conferences they wouldn't disagree with me. they would agree with everything i am saying, they're talking about this but they are terrified that they have one foot in this fee-for-service model and getting all these signals in this value model and don't know how to make the transition. it is a classic economic transition problem and the business model transition problems that you can be so comfortable, your state employee benefit program could be a leader in this, medicaid program could be a leader in this. >> what happens in this consolidation that can be consolidated way or the lowest cost hospitals because in a world where the strong survive, the ones with the most commercial patients? >> that is where the global budget tears. an episode care payment we pay for every little piece in a piecemeal way. would you can do is save for 30
7:29 am

days before hospitalization and all the rehab afterwards six weeks afterwards we give you one price but we fragmented the market so much is hard for one payer to take the lead on that and government can play an important role because you get in front and say our medicaid plan will play -- we will move to a global budget and the rest of the marketplace would follow. you have to pull a couple webers at the same time, encourage consolidation to change the way the payment happens. >> the idea of global budgeting in the same region i am from hawaii so the phenomenon we have of actually separate islands and the majority of the population concentrated on one island versus others doesn't necessarily fit so easily but the rural urban construct does. how do you differentiate -- wrong way to put it.
7:30 am

how are you incorporating into what you are suggesting the idea of urban versus rural? the capacity in the rural areas where you have a very high percentage of older people in hawaii right now and i suspect in one variation or another all the rest of the states the number of people over the age of 60, 65 is increasing. .. >> how do you take that into account where rural areas simply
7:31 am
do not have even some of the basic capacity, and you have to transfer people geographically in order to get basic services, especially as we have an aging population? >> there's a wonderful model in south central alaska. all the most interesting health care models are all in the middle of nowhere. they're not academic health centers. there is a stem in the middle oe in alaska. it's in danville, pennsylvania. it's camden, new jersey, you know? it's at the edges of the power structure. so i think the answer to what you're describing is a very structured intervention which is enough to keep people out of the hospital and also begin to have the hard end-of-life discussions. we don't have to ration health care, all we have to do is
7:32 am

deliver great health care every day that's truly patient-centered, and the rest will take care of itself. if you explain to people what's really going on and you build a relationship with them, all of these other discussions take care of themselves, so -- >> just one further element in that. could you discuss for a moment the relevance of hospice care in this context in. >> extraordinarily important, and i think a big part of the outcomes in the doylestown data set were the connection they made with hospice and having the time to sit at the kitchen table and really build a relationship with someone and with all the family members to be able to have those discussions. you know, you can't do this in ten minute busy, primary care offices. we have highly-paid professionals running from room to room to room in ten minute
7:33 am
encounters, meaningless encounters. that's what we're paying for. >> does the hospice idea include your idea of the patient-centered health care which we're trying to implement, i wanted to have that include patient-centered hospice be at the end too. you don't necessarily have to go to hospice, why can't the hospice be in home, if you will, with the visiting people. does that make sense? >> i think hospice is that. i think one of the most patient-centered services in america and the most brilliant service is hospice, and lots and lots of hospice patients die at home, they don't die in facilities. that's really the core mission of hospice. i think hospice, frankly, is way out if front of us. a lot of people don't get referred to hospice until a couple days before death because the doctors are uncomfortable having the hard discussion because you can't have a hard discussioning in a ten minute -- discussion in a ten minute
7:34 am

visit. >> well, do you have something to -- >> with respect to what you showed, is there a difference between for-profit hospital ands not-for-profit hospitals, and is one group getting it faster than the other? >> you know, i think that's a broader question, and to me, it's immaterial. there is good behavior and misbehavior on both sides, and, you know, there's an argument about managed care versus fee-for-service. someone has to manage a risk, someone has to pay claims. i don't want care who does -- i don't care who does it, do it well. someone has to run a hospital, just do it well. i think we've had the wrong argument all along which is you can make any system work if you have the right expectations, if you manage it well, if you have transparency of data, public reporting of data. >> but it would seem that the for-profit hospitals are taking the leadn consolidation
7:35 am

uh-huh.y. >> okay. >> you know, i think they're seeing the forest for the trees, and, you know, local hospitals have local boards. it's local business people, it's local attorneys, and no one wants to give up local control. the problem is these tiny little hospitals don't have the layer of professional management and professionalism on the board to really run a complicated hospital. so that when i go around the country, the very large systems i interact with are doing incredible work that you can't do until you get to a certain size and scale. >> yeah. could you give us a little primer on some of the language for consumers of health care that would help move the ball down the field? i mean, you think about the example you used about blockbuster of netflix, whatever, i mean, consumers ultimately made that choice as to whether or not to spend that hour and 15 minutes or to figure out how to do it some other way. it required a little work.
7:36 am

but what -- because it seems like we're talking a lot about the business, obviously, and the systems and what not. but ultimately, you're going to need consumers to be empowered inside the system to help drive decision making to the right place. what sort of language or discussion -- because i think there's, i mean, regardless of the level, i mean, some of the most incredibly unempowerred consumers in our world are people that are sick or hurt, and all of us have had that where everybody hears long lines or which doctor to try to see, which therapist, all the various work arounds you talked about before that we use. but what sort of language do you think can be empowering and motivating to individuals that'll assist us in getting the market-driven kind of solutions that we're talking about? >> i'm going to say a really sad thing, it's skepticism, and let me say why. there's a very famous study that
7:37 am
looked at knee surgery. the average patient is 40s to 50s, they're overweight. they've had swelling in their knee, pain for a couple week. they go in to see their primary provider, they eventually get an mri, and it shows wear and tear on the knee. what they did is called a sham. you got randomized to either having the usual procedure or to having scope where they just put it in and take it back out, and you wake up with a band-aid, and you have no idea which group you're in. they got better at exactly the same rates. we do 650,000 of these surgeries a year, and what happened is medicare set a really high price for it, and everyone raced to do it. and we built capacity, we put up billboards, and then we ran out of sick people. and then we worked down the
7:38 am

continuum to less and less and less sick people. so this was a brilliant thing. the fact that we can put a scope in and repair your knee is incredible. and be it works if you're an athlete. if you're 25 and you have an acute tear, it's incredible. if you are 250 pounds and 45 years old and have wear and tear on your knee, it doesn't work. if i took any of you out of work for 12 weeks, put you in physical therapy three times a week, told everyone in your house to take care of you, you'd all be healthier at the end of 12 weeks. that's why they get better. [laughter] so there are examples all across the health care system of stuff we're doing that doesn't work and hurts people. so there's a famous study that looks at an yoplasty, and if you have an acute heart attack, it's a miracle. they took stable heart disease and randomized you to a stent which is medication management, controlling your blood pressure, controlling your cholesterol. they got better at the exact same rate. so what happened was we stented
7:39 am
heart attacks, and then we ran out of heart attacks then we started stenting 80% blockages, 70 president block -- 70% blockages. you know, we built the wing, we hired the -- we overpaid for the local cardiology group. now they're onboard. fill the beds, you know? so we use off-label use of our own technology. so it's that conundrum where we're the most amazing health care system in the world because we can do all this cool stuff for people, and then we're doing too much of it unnecessarily. >> dr. brenner, you've hit on an a issue that a lot of us have thought about, and that is, you know, unnecessary procedures. i believe that probably doctors like yourself are the most trusted people in our communities. everybody looks to a doctor with great respect and reverence. you go there, you say take care of me, doc. i don't feel good here, i've got a pain there, tell me what to
7:40 am

do. you know, we have too many scopes being done on knees that are maybe inappropriate, too many hysterectomies we've heard about in the past, we have doctors that are doing preventive medicine because of legal issues and liability concerns. how can we get to a point where the doctors are doing the right thing for the right reasons not just incentive because, well, one more procedure here, i can get that done. i'll be careful, i'll give them another procedure, i'll get paid. that's the concern some have with profit, not for profit can we there's the doctors and the hospitals -- can we trust the doctors and the hospitals to do the right thing for me and my health as opposed to being motivated by something else? >> we have destroyed the american health care profession, and its professionalism has
7:41 am

eroded like many fields in america. so let's be clear who sets prices in health care. there's a committee called the ruck, and it's a subcommittee of the american medical association. they meet four times a year in zag, and they disease the rell -- in chicago. there are about 15,000 prices in medicare, and they make a recommendation to congress about how the prices for medicare should work. and 90% of the time medicare's taken their recommendations. and it's a committee of doctors setting their own prices. and the codes attached to those prices are copyrighted and trademarked by the american medical association. you can't download that and even look at it. you've got to pay for it. so the way that medicare and our country pays for all the doctor bills is copyrighted and trademarked by the trade association that sets its own prices. i mean, that's a stunning thing. and if you look around the room, docs, and the rest aremary care
7:42 am

specialists. so they set a very high price if you localize, a very low price if you talk to someone. and when you go to negotiate with aetna, you say i want 125% of medicare fees, and they say, no, we'll give you 110 %. it dose back to the origins of medicare that to negotiate, they agreed to usual and customary charges. and incredible bias is built into that fee schedule. you guys could correct that in your medicaid system, in your employee health plan system. you could begin to send a signal back up to the federal government that you're not going to tolerate the biases built into that schedule. >> [inaudible]
7:43 am

>> so many of our physicians in our hospital, you know, they practice protective medicine because they're afraid all the time of they don't do something, if you don't run a test, if they don't take advantage of everything that they've been taught, well, we're going to have those lawsuits coming upon them. what role does tort reform play into all of in this. >> so we have a perfect study in which 50 states you could track health costs, and some states like texas have set very severe caps. and they have not seen lower trend lines because they set the caps. so it's absolutely true that doctors practice defensive medicine, it's true that we need changes. that's all true. it won't fix the cost trends. the cost trends are because of unnecessary capacity, it's because of irrationality in the system, it's because of, you know, delivering too much of the wrong kinds of services.
7:44 am

so, you know, you have lots of -- you know, the ama's answer to this and physicians' answer to this is always tort reform. and you can say, you know, yes, you're right, the tort system need to be fixed, but that's not the answer to the cost trends. >> well, thank you, dr. brenner. that was incredibly interesting. [applause] >> thank you so much. ms. . [applause] >> that, i want to ask dan, our nga executive director, to give us an update of the work on the association in assisting states to control health costs while maintaining quality. >> thank you. you probably won't be surprised to know we're trying to emulate much of what jeff is doing. we actually have an agreement with jeff in trying to utilize his techniques. many of you know we have just awarded seven states' projects to see if we can take some of the techniques jeff and his
7:45 am

colleagues have developed and apply them to a state, see if they can be replicated and scaled up. we think it might work, so we're working with those seven states n. the meantime, we're also working on pieces of what jeff has done that we'll make available to everyone, things like software to identify the most expensive patients. we can provide that to you for free. so we're looking at other pieces of this that we can replicate and distribute as well. work force, we've mentioned how much we're working on work force. many of the folks who work with jeff are community medical personnel. and we don't really have a definition of what the community medical worker is. we don't have a training program that's recognized. we don't have a certification program in most of your states. and so there are things that work force really need to work on to rep hi candidate or at least use some of these techniques. we're also working on payment system reform. what does it take to gather the payments together the way jeff has done from various parts and
7:46 am

pieces of the system to be able to then repartition them. and that brings up an issue we haven't often dealt with which is antitrust. it's ironic but nonetheless true, as jeff said, they're not really competing for market share in these expensive medicaid patients, and yet the department of the federal trade commission was quite interested in what they were doing, and new jersey passed some laws to help codify some of what jeff was doing. regulations were written, and the ftc demanded to look at them and made some changes, ultimately negotiating with the state. but as we get consolidation, whether you think of monopoly-like positions or whether you are working down in the trenches like jeff, antitrust is going to become a much more important issue across the health care system, so we're trying to work with the ftc to see if we can get some guidance on how they will think of these
7:47 am
superutilizer ie're going to work with a number of your state, and in the meantime, we will have parts of this system that we can offer to all of you as we move along. so part of the answer, governor, to you que of can jeff come to iowa, i'm not sure he can, but we can. we'd be glad to do that. so we're going to be duplicating this work to the extent we can. we're also about to release a compendium of best contracting practices. much of what jeff talked about we can actually replicate contracts whether it's for medicaid patients or whether it's for employees and retirees. and the compendium looks like this, so it's about eight chapters of pieces of the contracting process that you could employ to require transparency or look at other aspects that jeff mentioned. data reporting, of course, those kinds of things. we have a couple of contracts that have much of this already. arizona is, i think, is one, tennessee's another. so there will be full contracts as well to look at, but we've
7:48 am

also torn them apart and written chapters of how you set prices, how you risk adjust, and you can do a fair amount of it by just managing contracts. we are also doing work, of course, in specific health areas. child health is important to all of you, of course, and we'll continue to see how we can do better at ma term and child -- maternal and child health. almost half of the births in the country now are financed by medicaid, so you have a big interest financially and health concerns of how maternal and child health fares in your state, and we continue to work on that as well. we have struck a deal with the institute of medicine that we're going to begin holding some statewide retreats. the basic notion is that a iom will bring to a state or within the state the health care side of the -- [inaudible] and you as governors can bring the political policy side of the
7:49 am
state. and we'll essentially spend a weekend in a room talking about what the state, the barriers are in your state to true reform and try to get a better sense of the answers to phi or six -- five or six critical questions. we're not going to answer those questions, to be sure. but the real prospect is we'll find at least what some of the big impediments are, what the data needs are, and we'd hoped to be able to jump-start, therefore, some of the reforms you have underway in the states. the parallel you're doing with grants and other things. our test case is going to be the state of wisconsin in october, we'll do the first retreat here. if any of you know harvey feinberg who runs the iom, you'll know his enthusiasm. he said, let's do ten states. i said, harvey, let's do one. if so, we'll be back to you on whether you'd like us to try and do this exercise in your state or not. so we're working from the top ethereal gas level all the way
7:50 am
down to some of the things jeff does every day to see how we can replicate this work, how we can expand it and how to make available to you more analytical tools, more knowledge of how to reform the health care system. you all have data. you have medicaid data. if not, you should get it. you have data on your employee populations, you have data or can get it on your retiree populations. the largest purchasers of health care for of you in your state. and so you can move a lot of material around. as i bored you back in february, states have many, many levers to pull. you control the entire spry of health care in -- supply of health care in the state, you have antitrust powers, pressuring powers, and by deploying those in good ways, you can actually change the system with some rapidity. so we're hopeful to be able to help. we had 24 or 5 of your governors' health advisers in washington earlier this week to begin getting them to talk to
7:51 am
each other asit was the first te ever had all the health advisers together at once, and they've begun those discussions and share what they're working on. equally important, learn what we might have to offer them and importantly, too, for them to tell us what you need. we may not have guessed right in some cases. but i think if we can take successful experiments, if you'll let me call it that, jeff, and test them other places and see how we can adopt them to both your state and to local health practices, we can begin, i think, to advance advancemente of -- advance. some of you are already testing other models. so the whole point of the health care exercise is you guys have a lot to do with it, and if you will decide to do so, we're happy to help you try that. and as jeff said, governors have a lot of say over how health care's delivered in their state, so we stand ready to help you with that. >> all right, dan, thank you very much. we are going to be in nashville
7:52 am
next summer for the 2014 summer meeting, and i'm going to ask the governor to come up and -- there he is. >> so i'll make a deal. if y'all will come to nashville, i promise not to sing now or then. [laughter] [applause] yeah. if you heard me sing, you should have clapped louder. we are excited to invite you to nashville 2014. nga will be there next summer be, july 10th-13th, and everybody knows nashville is music city, and we intend to entertain you appropriately with world class musicians. we'll go to the ryeman auditorium, the grand ole opry, but nashville's so much more. we were just recognized as one of five cities you should go to in the world before you die, and since the next closest one is paris, i suggest you come to nashville now.
7:53 am

but bon appetit named it the south's tastiest and coolest city, and rolling stone named it the best city for music, and even the new york times called us -- it's the u.s.' it city right now. so i can promise you, you will have a wonderful visit in nashville. we also have a lot -- the discussion we just had, more hospital beds are managed out of nashville than any otherty in the u.s., and could you can comd decide for yourself the impact on policy. we also make 300 million m and ms every day and sell jack daniel's whiskey along the way. so we have a whole lot to entertain you. and for those of you who are thinking, well, identify checked out the politics -- i've checked out the politics of tennessee, and some of you might say it feels a little red, we're going to have dinner one night at the hermitage, andrew jackson's home. and there will be two things that republican or democrat will reassure all of us that nothing has changed. his home contains more items of
7:54 am

his than any other presidential home including the newspapers that he marked up every night. and it will give you great reassurance to know that nothing has changed in terms of politicians' views of the media. his remarks are fairly blunt, i'll just put it that way. and the second thing is you can hear about jackson and those who think that politics has just recently turned nasty, when jackson was in his last days at his home and someone came and interviewed him and said do you have any regrets, and they were thinking this is his chance to be a statesman because he's long since retired from the presidency, he's in the last stage of his life, and he said, yes, i wish that i had shot calhoun and hung clay. [laughter] well, calhoun was his own vice president, so you can see how things -- [laughter] regardless, we promise you both a fun and entertaining and educational time, and we look forward to seeing you next july in nashville. thanks. [applause]
7:55 am

>> did you say bourbon and m and ms? [laughter] at each summer meeting, we take a moment to recognize our corporate fellows. all the governors know that we have a wonderful relationship with our, the fellows, and we very much are appreciative of their commitment to nga and their commitment to working with all of us. and as many of you know, this program really facilitates the exchange of ideas, in ways the corporate fellows are the thought partners with us in terms of improving public policy. and we want to take this opportunity to recognize a few of them. and i'm going to ask governor fallin to join me up here. governor fallin is the chair of the nga center for best practices, and she's going to help me recognize some of our longstanding companies. this marks the 25th anniversary of the corporate fellows program. back then there were about a
7:56 am

dozen companies, today there are more than a hundred, and one of these companies has been a member since the beginning, and today we recognize a founding member of the corporate fellows program. that is at&t. we are very appreciative of this partnership over these many years. [applause] and i'm going to ask wayne font to, please, join us here. now you can applaud. [applause] >> thank you. and this is this awesome picture. i'm assuming these are the -- who are these? >> who are they? [inaudible conversations] >> it is the original group. all right, that's great. is there a camera? okay, right here. mary, come on. [inaudible conversations]
7:57 am
>> thank you very much. [applause] >> we also want to recognize a few companies for 20 years of service. the first one is merck. saul, come on up. [applause] [inaudible conversations] >> thank you. >> and there are a couple companies we want to acknowledge that could not be with us, one is ford motor company, the other is fmc. we are very appreciative of them as well, and i know that all the governors join me in expressing our gratitude to them. [applause] that concludes our, this plenary
7:58 am
session. committee meetings are starting soon, and we look forward to seeing all of you over the next few days. thanks very much. [inaudible conversations] [inaudible conversations] [inaudible conversations]
7:59 am

[inaudible conversations] [inaudible conversations] >> you're watching c-span2 with politics and public affairs. weekdays featuring live coverage of the u.s. senate. on weeknights watch key public
8:00 am

policy events and every weekend the latest nonfiction authors and books on booktv. you can see past programs and get our schedules at our web site, and you can join in the conversation on social media sites. >> you're watching booktv, 48 hours of nonfiction authors and books every weekend on c-span2. here are some programs to look out for this weekend. at 1:30 p.m. eastern, booktv brings you the 20th annual eagle forum collegians summit. hear from several authors. for a complete schedule, visit us online at booktv.org. then tomorrow at noon it's your chance to talk to ben carson. dr. carson, the author of five nonfiction books including "gifted hands" and "america the beautiful," is live for three hours answering your questions from facebook, twitter, e-mail and by phone. watch these programs and more
114 Views
IN COLLECTIONS
CSPAN2 Television Archive
Television Archive  Television Archive News Search Service
Television Archive News Search Service 
Uploaded by TV Archive on
